[Image: closeup of a mock US one dollar note which reads “IN GREED WE TRUST” instead of “IN GOD WE TRUST”]
This blog post is for parents deciding whether to teach Sign Language to their Deaf children. If your child doesn’t have Sign Language there is a 1/3 chance they will end up PLD.
Roses are red,
Violets are blue,
You learned language effortlessly,
Deaf kids should too. Kimberly Sanzo
Please don’t misunderstand me. I’m not saying a cochlear implant program (CIP) is bad. I am saying that you don’t need to rush in. Don’t be pressured by lies. This is the most important decision you will ever make for your child. The research shows that all Deaf babies, including CIP babies, do best with Sign Language. Please don’t gamble with the decision. Don’t let the “experts” make the decision for you.
As Kimberly also says – As a parent, would you rather struggle to keep up with your child’s fluent language or watch them struggle their whole lives to keep up with yours?
When I spent 56 minutes watching a youtube lecture by psychologist Ann Geers (transcript) many things fell into place for me. She’s at the Dallas Cochlear Implant Program in Texas USA. If you’re not a statistician it will be hard. But sit down with a pen and paper and take some notes. The other inspirational video is, of course, Rachel Coleman’s video about Leah.
In Ann’s video, count the number of times she says the word “deaf”. Count the number of times Ann says “We’re not sure what’s going on.” Especially listen to the questions at the end. The one from Debbie Moncrief of the University of Pittsburgh might point the way to new research. The other question from the Speech Therapist made my blood boil. Basically they are not really evaluating what they are doing.
In the meantime I think there are five big lies you may come across.
1. Big Lie Number One – babies with early implants do better
Ann’s own data shows that ONE THIRD of babies with cochlear implants are still behind their hearing peers by the age of 10. It makes no difference if this third has had early implants.
Anti Sign Language advocates spread the lie that Ann included Deaf babies with additional disabilities. The fact is that Ann’s study says her data is from “normal” Deaf babies who have no additional disabilities.
2. Big Lie Number Two – babies need to be implanted early to learn spoken language
Rachel Coleman’s daughter Leah proves this is wrong. Leah is deaf and she learned to read and write English BEFORE she got her implants. Ruth Campbell’s research says “we suggest that the best guarantee of good language outcome after CI is the establishment of a secure first language PRE-IMPLANT [my emphasis].”
3. Big Lie Number Three – Sign Language interferes with learning spoken language
Often people will say there’s not enough research about this. I think there is. Kathryn Davidson showed this lie was wrong. She studied bilingual bimodal deaf babies with cochlear implants (ie they grew up with native Sign Language with their Deaf parents and learnt English at the same time). She said the kids “exhibited strong and widespread success in spoken English language skills. .. bilingual CI participants performed at monolingual English age target, and not significantly different from their hearing bilingual KODA peers.” KODA means kids of deaf adults.
4. Big Lie Number Four – we can’t predict if cochlear implants won’t work
Ann’s own work, strangely, shows this is wrong. Check out the Lexical Neighborhood Test (LNT) values for the Persistent Language Delay (PLD) kids. LNTs are lists of words read out in spoken English. Compare the PLD kids’ LNT scores to the other kids – the NLE kids (normal language emergence) and LLE kids (late language emergence). What do you notice??? It hits me like a brick in the face. At 50 dB they fail more than 50% of the words. Their scores at 70 dB are also much worse than the other kids. So even with a CIP, these kids are DEAF. They cannot hear the softer sounds in spoken language. They miss out on more than 50% and have to guess what they are hearing.
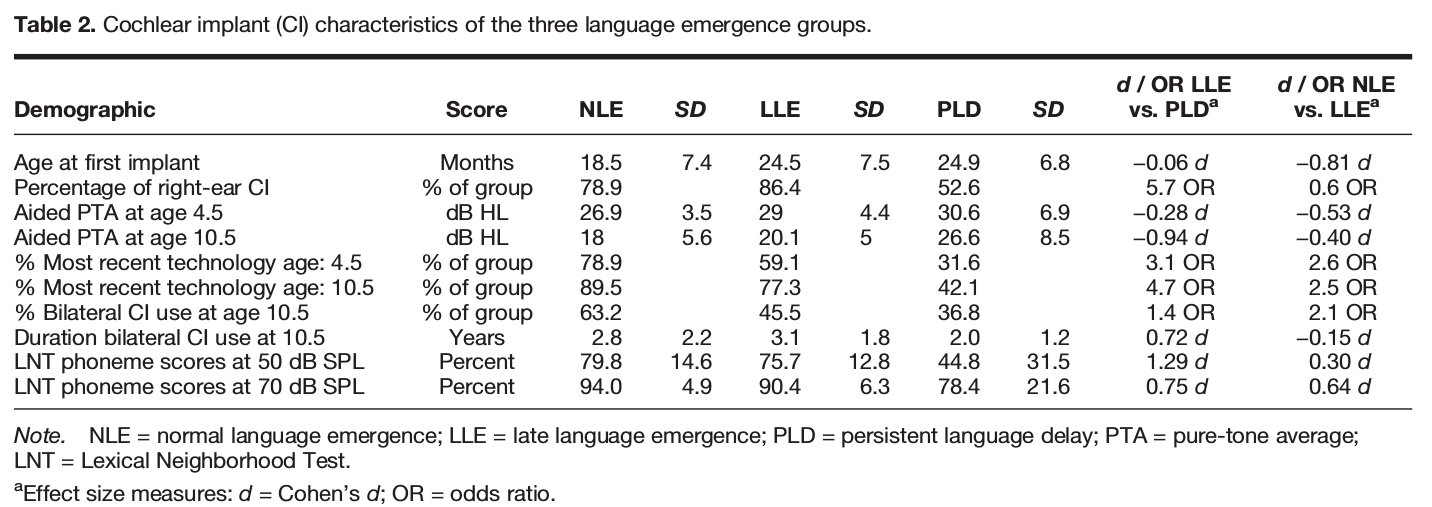
Source: Ann E Geers, Johanna G Nicholas, Emily A Tobey, Lisa Davidson, Journal of Speech Language and Hearing Research 59(1) October 2015
DOI: 10.1044/2015_JSLHR-H-14-0173
Persistent Language Delay Versus Late Language Emergence in Children With Early Cochlear Implantation
5. Big Lie Number Five – only a small number of cochlear implants fail
Lie Five is the biggest lie – only a few CIPs fail. What do we mean by “fail”? Even some Deaf people misunderstand this. There are two meanings of fail.
1. The CIP industry says only 1-3% of CIs fail. They mean technical failure of the CI or an infection. They don’t mean when the CI operation fails. My Deaf friends tell me of deaf babies dying on the operating table [later edit: I haven’t found evidence of this and other Deaf friends say it’s an urban myth. I’ll leave it here to acknowledge the error] . The popular belief (again without evidence) is that only 5-10% of CIP babies never learn to speak adequately.
2. The second definition of fail is even more important. It should be the major thing that parents think about. The failure is when a child can’t properly communicate with a spoken language even with a CIP. As we’ve seen above from Ann’s work, this is about 33% – one third!
The other vital conclusion from Ann’s video is that if a kid is not speaking reasonably well by age 3, they are very likely to be in the group that doesn’t catch up. Ann calls them Persistent Language Delay (PLD) babies. I call them Deaf. If their audiogram is bad and they are far behind their peers, they are unlikely to catch up.
In answer to Ann’s constant statements of “We don’t know what’s going on”, my wife Joanna said: “These babies are DEAF. They need Sign Language.” Yep!!!
The good academic overview in the British Medical Journal’s Journal of Medical Ethics is worth a read. The overview certainly belongs in an Ethics journal because it also exposes the lies. In particular the rubbishy “science” mixed with opinion in footnotes 2 and 3 stunned me.
Finally, don’t just take my word for it. Do your own research and listen to words of Ms Mairead MacSweeney of the Deafness Cognition and Language Research Centre in the UK. The science is clear: babies need strong sign language before they consider a CIP. This is exactly what Leah’s parents did. This is exactly what more and more parents in the Deaf community are doing.
Good luck with your decision.
BTW, the best place to get science research is Sci-hub. You can’t just enter words into sci-hub. Usually you have to know the exact title of the paper. Even better is to know the DOI number. People who don’t want you to use Sci-hub have forced them to change web addresses. So if the link doesn’t work, hunt around and check their twitter for the latest link @Sci_Hub

This is pro deafness agenda. Very biased and distorted.
LikeLiked by 1 person
Very biased, I have a 5 year old ci recipient and according to her teacher, she is. ahead of her class in spoken language, not only in words but actual vocabulary, if you did not know about her ci’s you would never know she is deaf.
LikeLike
40% of deaf kids have additional disabilities and unfortunately many of those kids will have trouble learning ANY language, including manual ones. Autism Speaks funded research on deaf kids with autism being raised with ASL as their primary language. 1/3 of them were the equivalent of “non-verbal” in ASL, which is the EXACT SAME PERCENTAGE of non-verbal autistic kids with typical hearing.
I did “baby sign” with all 3 of my kids and the one who never learned it is the one with autism, even though she was the one I most wanted to be able to sign since she had a speech delay. She later experienced progressive hearing loss and while she has done amazingly well with her speech perception post-CI, she still has language delay. She has not had any language testing since the CI so I don’t know her percentiles but I’m pretty sure that she would fall into the 1/3 of kids outside the normal range. However, she was outside the normal range for language back when her hearing was totally within typical limits. The issue is not that she can’t hear with the CI but that her brain has difficulty learning language because of the autism. Her cheerleading coach is an ASL Interpretation major and was teaching the girls some signs. The typically developing girls on the team were picking them up easily but my DD was struggling the same way she struggles with learning spoken vocabulary.
The good news is that the language delay does NOT mean that she cannot communicate effectively verbally. She may not be within the typical range for her age but she is perfectly understandable. “I goed on a airplane last morning” may not be something a typical child would still be saying at 8 y.o. but the meaning is clear.
LikeLiked by 1 person
Do you have a Cochlear Implant? Do you have a child with a CI?
You may have opinions yet, when your opinions clashes with facts, it renders your post as being biased.
I’m a deaf adult with a CI (received it two years ago) and l am also a life long culturally deaf individual, born to deaf cultured parents and raised with other siblings, all whom are deaf/hh within deaf culture. I clearly saw your post as being very biased.
You still have so much to learn about cochlear implant. Why would you write this post? My only conclusion is you may not be anti CI (as you have stated) but you are clearly biased because your opinions are not factually correct.
So, why are you writing this article? What do you hope to achieve?
The deaf community need to all come together and respect all choices, otherwise to continue this divide is only hurting the culturally deaf community further.
LikeLiked by 2 people
The author of the paper in point 3 is not Lisa Davidson (of Wash U in St. Louis), but Kathryn Davidson (formerly of UConn, now at Harvard). They have VERY DIFFERENT views about sign language, so it’s important to not confuse them!
LikeLike
Thanks. Corrected.
LikeLike
Thanks Gina. I’d be grateful if you could tell me which facts are wrong.
LikeLike
Thanks Crimson Wife, The Geers study was with kids with no additional disabilities.
LikeLike
Kia ora Danie. I’m really glad your child is going well. It’s the 1/3 of kids who don’t do well that I’m worried about. Can you tell me why that is a biased view?
LikeLike
Lou Ann, my agenda is clear. I’m pro-human rights. Can you tell my what part of the article was wrong?
LikeLike
“The Geers study was with kids with no additional disabilities.”
Why do you say this Kevin?
LikeLike
Hi Sym, Good to hear from you. The materials and methods section of her 2015 paper says all kids with “below-average nonverbal learning” were excluded from her study. She talks about them in her video too.
LikeLike
That’s the 2015 paper. The study quoted was 2003 from memory. I don’t believe the original group had “below-average” kids removed because at those early ages you can not identify most developmental issues. I also have not seen any discussion of this in the papers related to the initial and second assessments.
I wonder if you are looking at her new study group and imputing the attributes of that group onto the original study?
LikeLiked by 1 person
Alright, English is a THIRD language for me – Finnish Sign Language and written Finnish came first. I’ve refused to go to speech therapy and to use hearing aids, as long as I can remember (apparently I dropped one of those aids into the depths of our toilet bowl).
My parents did ask me whether I’d like to consider cochlear implants. That I don’t remember either, but they tell me I exploded in front of them. So yeah, no. It’s a matter of choice(s).
The choice of a language. The choice of the parents to learn a completely new one for their child. The choice of the child himself/herself. No matter the outcome, there is NO proof that sign language would in any way harm acquiring the written/spoken language. CIs are fine, as long as sign language is there. Bilingual (and multilingual!) children will only benefit the biodiversity on our tiny Earth, as sign language does in itself.
LikeLike
P.S. I’d be interested to find the source for that ‘40% of deaf kids have additional disabilities’ Crimson Wife referenced to? 40% sounds somewhat high. Thank you!
LikeLike
Recent surveys of the Gallaudet Research Institute (GRI) indicate that as many as 40% of children in programs for the deaf and hard of hearing have additional disabilities (GRI, 2003a,b).
LikeLiked by 1 person
I’m not sure what 2003 study you are talking about. In any case it would seem to be old science now that the 2015 has been published. No, I’m not imputing anything into the data that’s not there. 1/3 of “normal” deaf kids with CIs are language deprived.
LikeLike
This is the 2003 paper….
Click to access geers-lang-skills.pdf
…which has the finding that a listen and speaking only approach produces better language outcomes. It does not mention anything about removing “below average” children from the cohort.
Are you sure that the 2015 paper you are discussing is the same cohort?
LikeLike
Sym, I’d be surprised if the 2003 and 2015 kids are the same. The 2015 data didn’t include kids who were below average – I think that’s what you mean by “removed”. I think you’ve misinterpreted Geers’ 2003 paper. It said that the better outcomes were for kids with CI compared to kids with hearing aids. The very very sad facts of the 2003 paper also show there’s about a 50:50 chance that CI kids won’t have spoken English comparable to their hearing peers. Table 4 is a real zinger with appalling scores for the speech only interviews. The other interesting finding is that age of implant makes no difference. So the CI industry still pushing for early implant does so despite the evidence. This is immoral. The evidence is that establishing a strong first language, sign language, is best.
LikeLike
No. You need to read the paper again. Particularly…
“Use of a visual (i.e., sign) language system did not provide the linguistic ad- vantage that had been anticipated. Children educated without use of sign exhibited a significant advantage in their use of narratives, the breadth of their vocabulary, in their use of bound morphemes, in the length of their utterances and in the complex- ity of the syntax used in their spontaneous language. An oral educational focus provided a significant advantage for both spoken and total language skills.”
In terms of early implantation… you should read this paper (Aussie research)….
Click to access ching-et-al_-2009_-early-lang-outcomes-of-children-with-ci-interim-findings-of-the-nal-study-on-longitudinal-outcomes-of-children-with-hi.pdf
Particularly…
“Results demonstrated that children who received a cochlear implant before 12 months of age developed normal language skills and at a rate that is comparable to normal-hearing children. Children who received later implantation performed at two standard deviations below the normative mean.”
It is very important to understand that Geers work is set in the US context. The FDA discourages early implantation in children so the population she is studying has this impact. It is quite possible that this FDA guideline is generating the %age of children who don’t catch up. The Aussie study is important as it may raise this as a flag.
In terms of your conclusions here… I do think you need to be very mindful about how a parent who is coming to decisions about CIs reads this. This research is certainly not solid yet and there is much to be understood about what causes the 1/3rd of children in Geers work not to catch up. However the outcomes for children who get CIs, get two of them, get them early and take a Listen and Spoken Language approach are significantly better than those who take a sign language approach. While you say you are not anti-CI, some of your comments and conclusions could be interpreted otherwise.
LikeLike
Sym. We are talking at cross purposes here. You read it as if ALL children benefit. In fact ALL do not. The ones that do well are OK. The ones (1/3) who don’t do well are language-deprived. That’s unacceptable. Geers says repeatedly that she doesn’t know why the 1/3 don’t do well. It’s clear she hasn’t read her own data properly (not uncommon). The reason they don’t do well is that even with CI they are not hearing properly. Simple. As to the 2009 paper, Ching says the paper is preliminary only AND says the results are on average. Once again, it’s the 1/3 of kids that are missing out that I’m worried about. Averages, as we all know, hide a multitude of problems. And the problems in this case are fundamental rights to a language. Parents are unwittingly gambling with their kids’ futures. That’s wrong. There’s no need to gamble.
LikeLike
No. I am not saying ‘all’. I am very well aware of the issues around the 1/3rd. In fact you will recall that I introduced you to this issue in our discussions.
I do not think you are right that it is simply that the 1/3rd can’t hear. The children in these studies receive extensive audiological assessment and issues like poorly implanted CIs etc would be addressed. I also don’t think you can say that these children are language deprived. What you can say is that they are below average in their language assessments.
There are two obvious questions which then arise… why is this and would a different development language strategy help. There is no clear answer to either of these questions.
What is clear is that:
-predicting who is in this group is challenging currently
-adding SL has no positive affect on average (it may do for these 1/3rd but this is yet to be determined)
In terms of Ching’s findings, google the LOCHI study and see what they say about early intervention. If you are pointing to kids not being able to hear, then there is a very strong argument for younger and more cochlear implantation. Hearing aids are practically only effective up to 60db loss. The current criteria is 80-85db loss. There are kids stuck in no man’s land where hearing aids are ineffective (i.e. they don’t provide the critical consonant information). Now that is something to get really upset about.
By the way… you of all people should realise that with decisions like this there is an element of gambling. Most decisions parents make for their children are based on the best knowledge they can get. However there are always risks. Be it school choice, vaccinations, letting kids bike to school, etc, etc. Parents balance these things every day.
My concern here is that you are using emotive language (i.e. “5 big lies”). You are perfectly right to raise concerns. However there are no lies. There are some areas where there is currently inconclusive evidence (although in many cases there are strong indications). Added to this, there are strong refuting arguments… as I have already given… as to why your five issues are incorrect. My hope is that any parents thinking about CIs for their child will read your issues and then read the rebuttal.
LikeLike
Thanks Sym. The gamble can be eliminated by teaching kids Sign Language. Check out the number of deaf kids born to deaf parents who are language deprived. I dealt with the LOCHI study in my reply to you earlier. https://kmccready.wordpress.com/2016/10/29/cochlear-implant-dialogue-part-2/
LikeLike
The introduction of sign language does not eliminate the gamble. It just changes it. It introduces two issues:
1. That Geers study result impacts your child (i.e. lower language development results)
2. For most parents (95%+) it will lead to a language being introduced into that child’s life that is not rich. The idea that you only need to keep just ahead of your child’s language development is wrong. Children need exposure to rich language environments to develop nuance. Also once passed the basic learning it is all about context (you would know this from your book translation work).
You find a number of other papers regarding the LOCHI study post 2009. Worth having a look. It’s initial focus was around bilateral verses unilateral. The language side is now the focus.
I would again bring you back to Sarant’s conclusions that sign language isn’t a silver bullet but the evidence for what is isn’t currently available. That is a justifiable (and sustainable by research) message for parents. Anything more than that is personal bias.
LikeLike
I have three Deaf daughters. They all have implants but did not received them when they were babies. My oldest got hers around 10 years old. I was actually against the idea and she pushed for it. After deciding to allow it I have been pleased. HOWEVER, we still sign. They all have access to speech and love their implants but are so thankful that we sign. We not only share a special bond but they have amazing language skills. All three of them read well (my oldest is getting her MA) because they received language from the start.
I am obviously not against implants yet I wish parents would understand that it does not replace hearing. National Technical Institute for the Deaf did a great study. They showed that kids with CIs are not equal to students that can hear. On the contrary, the study showed that the students with CIs were behind their hearing peers and only a small percentage above their Deaf peers. Children with CIs do very well with speech. The problem is the that they miss incidental learning which is so vital for critical thinking skills and application of those skills later in life.
I become quite frustrated when children are implanted and the medical community suggests that the children should stop sighing. Funny that it is so popular and often recommended that parents of hearing kids should teach their children signs like more, please, yes and no, etc. There are so many article showing research that sign language helps kids that can hear get a head start on learning language. Why in the world would we say the opposite to children that cannot hear?
Here is the link below showing the study done at NTID/RIT
http://jdsde.oxfordjournals.org/content/19/4/471.short
LikeLike
Sym, you read my blog on LOCHI and Sarant. Sarant and LOCHI are secretive about their data and there are huge methodological problems with Sarant’s “metastudy”. The Geers results don’t show lower language outcomes for sign only. The effort for parents to learn sign is small compared to the effort kids have to put in with a CI. We need better ed for parents learning sign, not to throw our hands in the air and say it’s all too hard.
LikeLike
“Both age at implantation and length of implant use have been found related to various measures of speech, language, and literacy, including vocabulary (Connor, Hieber, Arts, & Zwolan, 2000; Dillon, De Jong, & Pisoni, 2012; Tye-Murray, Spencer, & Woodworth, 1995). Tye-Murray et al. (1995), for example, found that children who received their implants prior to 5 years of age showed greater growth rates in phoneme accuracy and word intelligibility than children who received their implants at a later age.”
“Earlier implantation was found to be associated with greater rates of vocabulary growth, with the youngest group showing significantly greater vocabulary growth for the first 3 years after implantation. After 4 years of implant use, however, the rates were essentially the same for all four groups, comparable to the rate of vocabulary growth normally observed in hearing children. “
LikeLike
Thanks Melissa. The 2000 study is now dated and did not look at Sign Language per se. The authors also said “The results of this study should be interpreted cau-
tiously and conservatively.” De Jong, & Pisoni, 2012 showed, again, 1/3 of kids were not performing to standard. The Tye et al study of 1995 is also small (N=27) and dated, but clearly said “Children who have more residual hearing, as indexed by puretone thresholds, usually achieve greater success.” This accords with the Geer data: ie profoundly deaf kids don’t do well with CI. Again, let me stress – 1/3 of CI kids don’t benefit from CI – they are profoundly Deaf and need sign language.
LikeLike
Kevin… you are really spinning the information in the research. NO ONE… absolutely no one has said that “1/3 of CI kids don’t benefit from CI”. I challenge you to show any research that says that. That is pure spin and COMPLETELY inaccurate. One could even say it is a “big lie” to use your terminology.
The research shows that 1/3rd of children with CIs don’t catch up and become age appropriate in language. That doesn’t mean they don’t benefit from having CIs. On average even this 1/3rd below average group do benefit immensely.
What the research does not answer is WHY this 1/3rd don’t catch up completely. Is it because they are part of the 40% who have additional developmental issues? Ann Geers is looking at this. Is it because they are implanted later than optimal? Is it because the support resources needed aren’t available? Is it simply that they would never have caught up because of underlying developmental issues? There are numerous possibilities.
Your default to saying sign language is the answer is an emotional one… without substance in research. At best you from the available research you could say it wouldn’t hurt (although you have to ignore some research to say this). You certainly can not positively that it is the answer from the research. If you want to argue for SL then you should be clear that you have an ethical, political and/or moral argument for it and make that argument. There is no clinical argument for learning sign language.
LikeLike
Thanks Sym. I need to be more accurate in my language. Yes some in the 1/3 may benefit but they are left “Persistently Language Delayed (PLD).” Geers’ research does indeed show why they are PLD. Check out their hearing ability even with CI – the data is in Geer’s paper. The PLD kids can’t distinguish the softer language sounds and consonants that are so important in minimal pairs. Yes I have a strong ethical stance: Leaving kids Persistently Language Delayed (PLD) due to total reliance on CI is immoral.
LikeLike
“Geers’ research does indeed show why they are PLD. Check out their hearing ability even with CI – the data is in Geer’s paper. The PLD kids can’t distinguish the softer language sounds and consonants that are so important in minimal pairs.”
I think you are inferring too much from a single line of data. You need to remember that Geers is a very experienced clinical audiologist and researcher (definitely in the top ten researchers for CI children in the world). If this data meant what you think it does, she would have dived down this route.
I do agree with you however that good mapping is critical for children with CIs to do well. I also would say that there is great variability in the ability of CI audiologists. Most parents figure out very quickly that good audiologist is worth their weight in gold. And conversely, a not so good audiologist will cost their child.
I also agree with you that it is immoral to leave a child in the “persistently language delayed” state where there is an opportunity for them to close the gap. Where we disagree is the strategy for doing this. I argue there is in adequate information to know what to do currently. You are arguing from what appears to be an emotional rationale that SL could help. However as Sarant said, there is no peer reviewed evidence to show that the addition of SL to an oral approach aids in language acquisition. And there is certainly no research to say that SL aids these kids in the 1/3rd.
LikeLike
Kia ora Sym. Thanks for a great response. I think we’re getting closer to an agreement. Many researchers, even the best, make mistakes and/or are unable to see the wood for the trees. It’s great to hear your critique of audiologists too. Have you written about this? Link? Joanna has found the same. Unfortunately the industry is set up to make money and now controls many audiologists. It takes a brave one to stand above the crowd and put people before profit. We actually found a deaf audiologist! Needless to say I disagree strongly with Sarant. There is lots of good data on bilingualism. The data on how the 1/3 can be helped is there too. Leah Coleman and others in this thread have shown that. The comments by Debbie Moncrief towards the end of the Ann Geer video were amazing also in that regard.
LikeLike
One of the important things about research is the peer reviewing process and reproducibility. Geers work has been reproduced by a number of other smaller studies. I would place a lot of trust in Geers work and her conclusions.
There is a bit of research on the quality of mapping. Much of it is around the CI companies trying to find an automated way of doing so. There is NRT and evoked potential approaches which offer some hope but don’t seem to be able to be refined. Vanderbilt University has been doing a large and seemingly successful trial on image guided mapping. The papers out of this work are quite interesting. This work shows that there is a real art to mapping. Some audiologists, like artists, are more gifted.
I don’t think profit and money drives the audiologists directly. I don’t think a deaf audiologist would be better or worse than a natural hearing one.
Yes there is lots of strong good research on bilingualism. The problem you have is you conflate bilingualism with bimodalism. Two or more spoken languages is a different beast to leaning a visual/manual language and spoken languages. Again, the research on bimodalism is limited but pointing towards negative. I think you are chasing shadows when you say there is data in the current studies to show bimodalism (learning both SL and spoken language concurrently) would help the 1/3rd who don’t close the gap.
My guess… only a guess… is that lack of auditory stimulation leads to other developmental issues. Paediatricans I have talked to say that it is next to impossible to identify many developmental issues until children are over 7yo (sometimes older). It is my suggestion that a lot of child development is sequenced and without the pre-requisite step, it tends to be difficult progress normally. Obviously there will be exceptions to this rule but would explain why the academic results on average for SL only students are so spectacularly appalling.
LikeLike
Syn do you have a study on SL only being “spectacularly appalling”. A paper quoted in this discussion showed only marginal difference between SL and CI.
LikeLike
The outcomes for deaf education have always been historically appalling. The outcomes now for kids with early implanted bilateral CIs who get intensive AVT are substantially better.
You may wish to read this overview paper which will give you some references to studies which show this…
Click to access language-outcomes-after-cochlear-implantation.pdf
LikeLike
Thanks again Sym. I’m always keen to get new info. The only mention in that source was unsubstantiated (footnote 37 merely linked to a literacy test, not to any results which were claimed in the text of the article). Interestingly the article was “Some children with CIs will learn to rely heavily on their listening abilities. For others, communicative competence will include the use of sign language ..” The old 1/3 again I guess. I’m still left wondering what’s the evidence for “appalling” English literacy of native signers compared to CI?
LikeLike
Some references for you…
“Historically, studies of deaf people’s educational attainment around the world have shown a wide gap between deaf people’s education levels and those seen in the general population (Barnartt, 2006; Bat-Chava et al., 1999; Richardson, 2001; Welsh & Macleod-Gallinger, 1992). To take two Australian examples, a survey of deaf students who left school in 1960 found that none of the 46 respondents had any postsecondary education (AAD 1973, cited in Winn, 2007), and the study of Bonser and Burns’ (1998) of around 850 deaf people living in New South Wales found only 7.6% held an associate diploma (2-year tertiary degree) or higher level qualification. In absolute terms, it is clear that deaf people’s educational outcomes are improving. In the United States, for example, Billies et al. (2003) note that the number of deaf and hard-of-hearing students in postsecondary education programs almost doubled in the 10 years to 2003 (cited in Richardson, Marshark, Sarchet, & Sapere et al., 2010), whereas Barnartt (2006) reports the proportion of deaf/hard-of-hearing men and women with at least some college education almost doubled between 1972 and 1990–1991. In relative terms, the data are more mixed. In a recent study of deaf people’s educational attainment in Sweden, Rydberg, Gellerstedt, and Danermark (2009) found that the attainment gap with the reference population was smallest in the 25–34 age group and increased in each 10-year age band. However, the overall gap remains significant, and the deaf population continues to lag the reference population 5%–21% in the proportion of people having undertaken 3 years or more of postsecondary education. Drawing on older data from the United States, Barnartt (2006) noted that while the rate of college education increased in the U.S. deaf population between 1972 and 1990–91, the increase was not as large as that seen in the general population.”
LikeLike
Thanks. Some interesting stuff. But the point I’m interested in is the literacy gap between native signers and kids with CI. The gap is not that big according to data referenced earlier.
LikeLike
I’m more focused on the education differential and corresponding income differential
LikeLike
I just came across this. I haven’t seen it before.
LikeLike
This article is quite interesting and as a speech pathologist I agree with some of these “lies” however some of the arguments this person has given are quite biased and do not seem to take any factors into account other than that someone has had a CI. It’s true that sign language does not impede spoken language development in fact in children with delays it can have positive effects on spoken language development. However it is crucial for implants to be done as early as possible for oral speech and language development. The key thing to note in this persons argument here is that they’ve said their daughter learnt to read and write, they didn’t talk about her oral language skills and we don’t base research on single subjects as they do not necessarily represent a large cohort of people in this population. I don’t know where this person got their dats regarding the statement that a third of children who have CI don’t develop speech. There is significant evidence that early implantation of CI increases the outcomes for speech and language development in children who have had implants in early toddler stages. This person hasn’t addressed external factors to hearing loss that people who have had CI may also experience, such as those who have speech and language disorders, intellectual impairments, troubled family lives, the list goes on for things that can impact oral language development for people with CI. Also the argument regarding predicting CI failure doesn’t actually discuss predictors of failure at all. I think that this is quite a heavily subjective article and the information in it should be considered with that in mind.
LikeLike
Thanks Bee. I’m glad you found it interesting. You make a couple of errors in your response. 1. It used to be thought that early CIP was important. It’s not. In fact logically one case can disprove something -the old “all swans are white” error. 2. Sorry I didn’t make it clear. The young woman’s English speech is perfectly understandable. 3. Data on stats is from Geers and the issue is PLD. 4. The Geers data is net of the other factors you mention (tough family life etc). 5. The best predictor is the audiology chart. Deafer means worse outcomes. I thought I made that clear. Sorry if I didn’t.
LikeLike
Some more research to add to the discussion…
http://www.news-medical.net/news/20170612/Research-shows-how-sign-language-exposure-affects-young-cochlear-implant-recipients.aspx
LikeLike
Thanks Sym. It fails to address the proof that it’s much better to establish sign language first and then LATER think about a Cochlear Implant Program (CIP). http://www.deafchildren.org.nz/assets/Resources/Hearing-Communication/Language-Choices-for-Deaf-Infants.pdf Language-Choices-for-Deaf-Infants.pdf
Clin Pediatr (Phila). 2016 Jun;55(6):513-7. doi: 10.1177/0009922815616891.
LikeLike
Actually that’s precisely what it does address.
it would be nice to see other researchers undertake the exact same research on bigger sample sizes. It would add to the certainty that mixing modes – especially in families with no SL background – is a bad idea. However there is an ever growing body of research that points to this conclusion. 🙂
LikeLike
No it doesn’t Sym. It makes the now disproven assumption that early CIP is better than establishing strong language (ie Sign Language) first.
LikeLike
I don’t understand what you mean???
You do realise the paper you posted has no clinical research to it. It’s what I call an “interviewing my typewriter” paper. In short it is an opinion piece. The paper I posted is a report on solid clinical research.
You of all people should realise that continuing to ignore the growing platter of data and instead pointing to opinion pieces with no clinical research to them lacks a degree of credibility. If you are going to throw terms like “Big Lies” you need to refute with solid evidence – not just opinion puff pieces.
LikeLike
Sorry Sym. I’ve now corrected my comment. What I meant to say was “now disproven assumption that early CIP is better than establishing strong language”. You may call it “interviewing my typewriter”, but that is a misunderstanding of how science proceeds. The paper you criticise is in fact an excellent summary of solid research. I am happy to change my ideas when presented with new data. For example, I have been working in the last few days on trying to put a better estimate for the number of Deaf kids left without a language. Initially I estimated about 50-60 per year (based on number of Deaf born per year then using Geer’s results that 1/3 are left language deprived. Do you have an estimate for the number and how would you derive it? Here’s my understanding of how science proceeds: https://www.youtube.com/watch?v=RxyQNEVOElU
LikeLike
Arh… that makes more sense.
I don’t think it makes that assumption. It provides real clinical data something your literature review doesn’t. While literature reviews have their place, they should be referencing empirical studies… not other literature reviews. This is the weakness of the research you point to.
Also… you are seriously suggesting delayed implantation? You are out on a limb of a broken branch with that one.
LikeLike
As for getting numbers… it’s very easy. There is the National Deafness Notification report. Use that. Or you can do 1 per 1000 live births for profound level hearing loss.
LikeLike
The numbers I’m looking for are of kids with PLD.
LikeLike
You won’t get that in an NZ context because there is no standardised testing across the spectrum. The DECs are meant to be doing this but don’t have enough people with the skill sets to provide norm referenced language testing.
Interestingly in the recent Geers data you can conclude that 1/3rd, 1/3rd, 1/3rd split isn’t that bad… especially for those choosing an LSL approach with CIs.
From my knowledge the only source of PLD estimates is Geers and maybe First Voice. However Geers work is set in the US and you have to be careful in using that data as their CI journey is different to Kiwis. The outdated FDA guidelines on early implantation and the health insurance incentive to do sequential implantation mean things are quite different.
LikeLike
Eeeek!! Up to a third of Deaf kids being language deprived is very bad. Yes. I’ve based my estimate as a third of the 170 diagnosed Deaf kids in NZ per year. How many of these PLD kids have you met?
LikeLike
If you rounded it to 180 to make the maths easy… 60 kids per year group with hearing issues who have long term language delay would not be unreasonable. 13 years of schooling so 800 odd kids floating in the school system with long term language issues.
The question is whether that is a significant number given the other issues like auditory processing, autism, physical development issues, behavioural issues, etc. I’m not sure where it falls.
LikeLike
It’s enormously significant!! I’ve met some of these kids. Of the ones I’ve met there is no rational reason for their PLD. How many do you think you’ve met?
LikeLike
I don’t disagree that it is significant for the individual kids. However there are other issues that are significant for other kids too – and lead to long term language delay.
I’ve probably met in excess of a 100 over the years one way or another. So only a drop.
LikeLike
Thought of you Kevin when I read this today…
http://www.aappublications.org/news/2017/08/03/Does-Early-Identification-Of-Hearing-Loss-Make-A-Difference-In-Language-Outcomes-Pediatrics-8-3-17
I know you are interested in such matters and appreciate the definitiveness of the American Academy of Pediatricans.
LikeLike
Thanks Sym. Are you aware that it is so flawed that there have been calls for it to be retracted?
LikeLike
Not by Paediatricians. But I will just leave you with this as it is from the chief editor of the AAP. It also represents the mainstream view point regarding the value of early intervention. Most would regard a contrary view to be quite extremist and certainly not fitting with current clinical evidence.
LikeLike
Sym, you can make wherever claims you like but they are not backed by science. What is extreme is an industry that refuses to address the human rights abuse that is one third of Deaf kids on CIP being Permanently Language Deprived.
LikeLiked by 1 person
What’s the %age of Deaf kids who don’t get early CIs with Permanent Language Deprivation?
As we have discussed there will always be a %age of kids with poor language outcomes. What we should all be searching for are the factors that reduce that %age. The factors that have solid evidence behind them are:
-Early Intervention
-Early implantation
-Bilateral Implantation
-High parental involvement
-Maternal educational achievement
-Not using sign language unless SL is the parental first language (it may also be not using it at all but that is less solid but certainly indicated)
-Use of music therapy
-Quality mapping
I want to make it very clear to others reading this discussion that the assertion that doing stuff “early” like intervention and implantation makes no difference is simply wrong and completely contradicted by the research currently available. And it has been for decades. And it contradicts the rule of thumb for almost everything to do with child development – that being earlier is better. Paediatricians, audiologists and other clinicians would be appalled at some of your assertions.
LikeLike
Sym I’ve posted enough evidence here for any intelligent person to draw their own conclusion. Your assertions are simply wrong.
LikeLike
I’m sure they will 🙂
LikeLike
Pretending bilingualism doesn’t work is like denying the moon landing. There are numerous cases where Sign Language has been learned first and English second. Pretending otherwise is bizarre in the extreme.
LikeLike
Really interesting reading all the comments here. symgardiner – thanks for bringing up how historically deaf education has done appallingly and for sharing substantial evidence on this. Are you also aware that from 1880 up till about 1990s/early 2000s, deaf education was mainly oral? That the German Method of Instruction (oralism) was implemented globally, wiping out sign language in deaf schools world over? In fact, sign language was banned globally post the Milan Conference in 1880 and oralism was decided to be the better method of education for the deaf. So you’re right in saying that deaf education has failed but I’d like to clarify that specifically, an ORAL deaf education has failed the Deaf community.
LikeLiked by 1 person